About the Author:
Mariano Mora McGinity was born in Newcastle‐upon‐Tyne (UK) and raised in the UK and Spain. McGinity holds degrees in Composition (Musikhochschule Düsseldorf), Guitar (Real Conservatorio Superior de Madrid), Philosophy (UNED University Madrid) and Journalism (Universidad Complutense, Madrid). McGinity is currently studying a PhD in the Media Arts and Technology department at the University of California, Santa Barbara.
For more information about all of the contest winners, please see the full contest winners announcement.
Participants in the competition warrant that their ideas are their own. Where ideas include component-ideas or materials by others, applicants warrant that any intellectual property owned by others and used in their submissions is approved for use and appropriately attributed.
The copyright or patent for any material submitted for the competition remains with the original owner.
Description of the Idea:
One of the greatest tragedies of the technological revolution brought about by computers is that, even to a greater degree than the industrial and oil revolutions, it hasn’t improved the living conditions of a vast majority of the world’s population.
In this paper we propose a simple idea that intends to do just that: contribute to improve the living conditions of people who have no easy access to technology. We introduce the main idea, explain why we think the idea is a good and perhapsa necessary thing, suggest a number of ways which might help to realize the project, and finally discuss what are the social benefits of carrying it out.
I.
The project consists of three main elements:
- A vehicle equipped with a satellite dish and medical equipment and medicines: for all practical purposes, a mobile consulting room.
- A medical networking website, where doctors can log in voluntarily and offer their expertise and effectively carry out examinations of patients through the Internet.
- A database containing the medical histories of all the patients who visit the health care vehicle. These histories would be made accessible, prior consent from the patient, to the doctor who is carrying out the examination, thus enabling her to make a more accurate diagnosis.
The basic idea is to create a tool that would make health‐care available to people who haven’t access to a health institution. The health‐care vehicle would effectively carry out the task that country doctors used to, and in many parts of the world, still do. It would travel throughout the region, visiting different villages or isolated houses at regular intervals. The vehicle is equipped with a satellite dish and digital cameras, thus making it possible to establish an online meeting between the patient and a doctor. The staff required for each vehicle is minimal: a driver and/or technical consultant, who could be able to connect to the website, and a person with the knowledge to manipulate the medical equipment (if need be following the instructions from the doctor) and help as a
translator to ease communication between doctor and patient. Naturally, only one person could fulfill both these roles.
They are assigned a password after they have accredited that they really are doctors, they are distributed according to their specialty, and, as doctors the world over who have ever worked ER, they wait for the patients to log on to the website. Once communication with a patient has been established and the patient has consented to show the doctor her medical history, the doctor
receives a copy of it on her screen. A normal examination proceeds via a digital camera and with the help of the vehicle’s staff, who can manipulate the required equipment. The results of various tests can be obtained within the time allotted to each patient. The doctor can then make a diagnosis if she feels confident enough, or consult other doctors who are logged in at the time, or ultimately
refer to another specialist. If a more serious intervention is required the vehicle can transport the patient to the closest hospital, however far that may be.
The database of medical histories can help to improve massively our knowledge of non‐western diseases. Cross reference of symptoms according to different social groups, origin or tribe of the patient, areas of extension of the disease, etc, could greatly benefit scientists researching to prevent and eradicate these diseases.
II.
We will not provide all the data in this short presentation that show how far we still are from the Millennium Development Goals proposed by the UN in 2001 and which are supposed to be reached by 2015, but rather leave it for our slide presentation. This project follows in the spirit of the goals in that it tries to provide universal health care for all people in the world. The main goals of
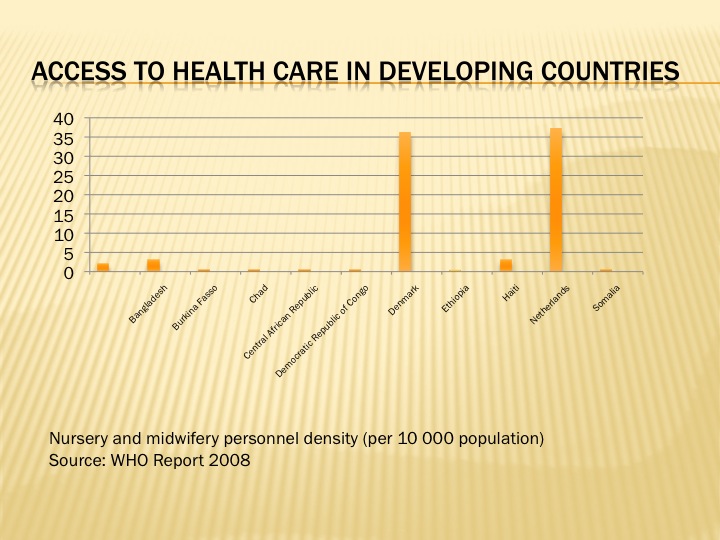
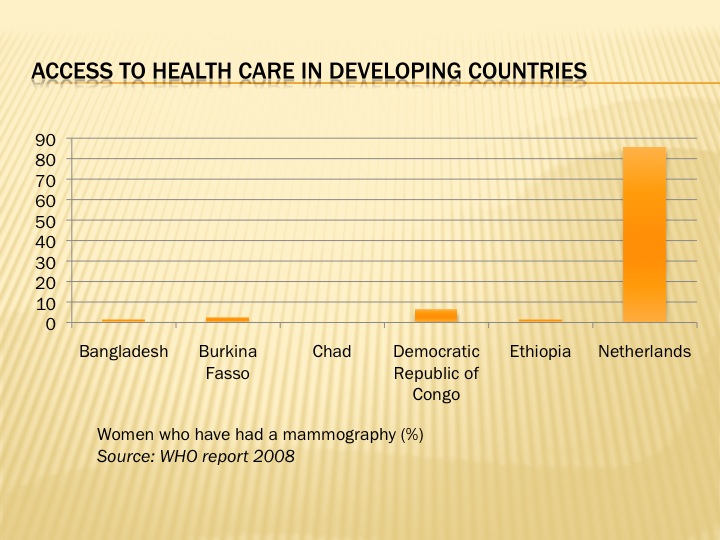
stopping the spread of epidemics such as AIDS and completely eradicating cholera and other poverty‐bound diseases can only be reached through a program that incorporates prevention and primary health care. In most countries, these are provided only through hospitals and medical centres, located many times many miles away from people’s houses. For a vast majority of the world’s population, a visit to the doctor is simply not part of their yearly routine, be it because of the distance they have to travel, their inability to pay for the visit (as well, of course, as the medicines), or simply because there aren’t any doctors in the region. Great efforts carried out by local medical staff as well as other organisations such as Doctors Without Borders has helped great deal in mitigating this need, especially considering that their work is mostly or completely) without retribution. But it is still not enough if we are to meet the goals of universal health care and eradication of epidemic diseases. Of course, the matters of health care and poverty are intimately bound, poverty brings with it diseases, but also, disease brings with it poverty, as we will discuss in out
presentation slides. Helping to eradicate one will also help to mitigate the other.
III.
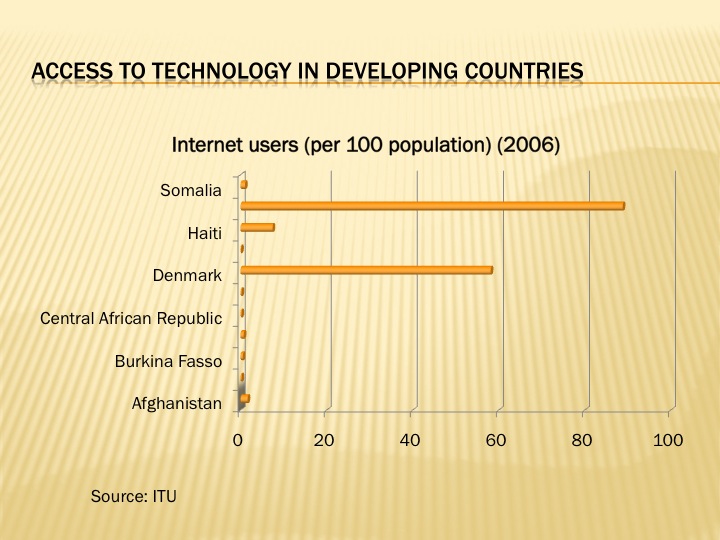
Some of the technological issues involved in this project rely directly in a much awaited improvement in land connections in developing countries. An example of recent development in this area is the East African Submarine Fibre Optic Cable System, supposed to be operational in the second half of 2010. EASSy should compliment other submarine communication systems such as SAT‐2 and ‐3, and finally link the east coast of Africa to the Middle East and the rest of the world. This will mean a huge improvement in the Internet access in the continent, softening the need to rely almost exclusively on geostationary satellite
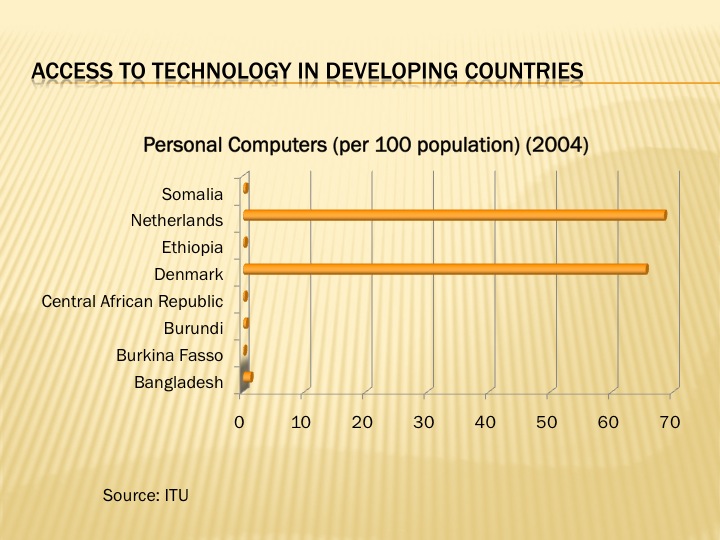
communication. Internet access is expected to grow exponentially within the next five years in Africa due to the realization of the system. Internet access nowadays, however, is another measure of the huge disparity between richer and developing countries. The image shows a 2005 estimate of the density of Internet use worldwide.
We will discuss this issue more extensively in our presentation slides.

Worldwide density of Internet usage (note the huge gap of China)
IV.
As we mentioned above, improving health services in developing countries cannot be distinctively set apart from helping to eradicate poverty. There are however many other social aspects that our project can contribute to, perhaps not as apparent, but also perhaps no less important.
Information exchange in many developing countries differs from what we have come to know as information exchange. In many countries, the information to which people could gain access through our system might prove to be vital for their survival.
- Where to find drinking water. This is especially important during draughts. It is also one of the Millennium Development Goals.
- Where to find other resources, such as cattle, favoured hunting areas, whether and where food is being distributed in all‐too‐frequent times of famine…
- One (or even better, a fleet of) mobile health‐care centre could prove to be extremely useful in countries prone to suffer from natural disasters. Their help in attending to the victims, transporting goods and becoming an on‐site information exchange centre, for the victims as well as for the outside world who might be making great efforts to organize aid, would prove invaluable.
- War is raging in many developing countries. Through exchange of information people can find out where the different factions are located and thus be able to avoid being caught in a battle zone, whether there is a risk of a raid, to search for family members who may have gone missing or been taking away by fighters…
- In almost all forms of cultures doctors (whatever that culture considers to be a doctor, a healer) have served a role of social cohesiveness, they glue members of that society together. A visit to the doctor fulfils a social need as well as a private one. Our project, the vehicle that goes from village to village, could prove to be a substitute in societies which have become fragmented through war, poverty, famine, natural catastrophes or the consequences of poverty: it would provide an opportunity for families to
talk to and see relatives who have to had to emigrate to another country or move to the city looking for the chance of a better future.
We believe that this project would be beneficial for developing countries. It would tie together efforts carried out by different NGOs trying to provide for health services and technology in countries that are lacking both. By bringing these two concepts together, the project could fulfill a role that, however humble, is not being carried out at the moment, and which might prove to do much good.
Imaginative Realization, Embodiment, or Illustration of the Idea:
CONNECTING DOCTORS AND PATIENTS IN DEVELOPING COUNTRIES: MOBILE VIRTUAL HEALTH CARE
by Mariano Maro-McGinity